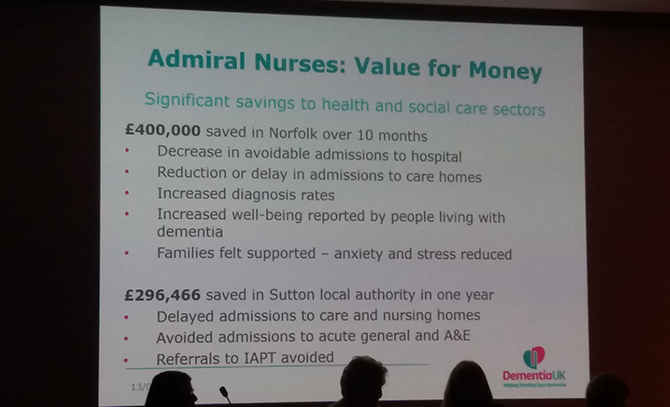
Earlier this month, I attended the Dementia 2020 conference, held at the Royal Society of Medicine; the slides you see here are a small selection from that event. The topics were wide-ranging and interesting, but a recurring theme that I welcomed was sustainability. This is something the Butterfly Scheme has always addressed and which I have been giving additional attention to in recent times; let me explain why.
When the Butterfly Scheme started out, dementia care in hospitals was rarely considered a topic worthy of particular attention. Some individual members of staff had insight and skills, but many regarded people with dementia as a problem, rather than understanding that skilled dementia care would remove or alleviate so many of the problems those people were facing.
As time went on, Dementia Leads were required to be named within hospitals – but note: these were people who nominally led in all things dementia, rather than whose active role it was to lead in dementia care. I’m very glad to be able to say that dementia care leadership is now an expected role – but which elements of dementia care leadership should the Dementia Lead be fulfilling? Leading a team? Yes, I would hope so! Leading the approach and scope of dementia care? Absolutely! Leading (and often actively doing) all the administrative work involved in every part of the healthcare team’s dementia care approach? Now then, that’s where we have to reflect.
Within the Butterfly Scheme, admin has always been kept to a minimum – but leading a hospital-wide care approach will inevitably involve some degree of admin. Again, within the scheme we have a structured leadership approach in each local team – but with inevitable staff turnover and an increasing pride within ward teams in their own dementia care delivery, how can the scheme support those ward teams without giving the local Dementia Lead more work?
What the Butterfly Scheme has been developing in recent months has been 1. additional ways of offering its established certification for those who can prove their ability to apply the scheme’s care, plus 2. ways for the ward teams to be able to evidence and develop the quality of their own dementia care delivery – both whilst actively reducing the admin required of the Dementia Lead. As with all things Butterfly Scheme, this has been developed collaboratively via regional liaison, so that the structure is exactly what the healthcare teams want.
Ask any Dementia Lead what they’d like to deliver and how close they come to being able to deliver it, and you’re likely to find that the workload has increased so much in recent years that they struggle to fully achieve any aspect of it. Often – and worryingly – instead of being given more time to lead dementia care, many have had additional areas of leadership added to their role. It’s time to take two important steps: to recognise the need for appropriately-sized dementia leadership teams, plus to reshape the workload so that it can be spread across a number of roles, rather than requiring the Lead themselves to deliver all of it.
So much is now achievable in dementia care – but it will only be successfully delivered if we ensure that sustainability is inbuilt.